In the landscape of modern mental health, moving toward measurement-based care (MBC) has transformed how depression is identified and treated. Central to this evolution is the Patient Health Questionnaire-9 (PHQ-9), a concise nine-item self-report tool that bridges the gap between a patient’s subjective feelings and objective clinical data. Whether you are a healthcare student, new administrative staff, or a patient seeking to understand your results, mastering the scoring process is essential.
The PHQ-9 is celebrated for its efficiency, typically taking less than three minutes to complete and even less time for a clinician to score. Despite its brevity, it is a “gold standard” screening tool with an 88% sensitivity and specificity for detecting major depression when using a specific cut-off score.
Prefer listening over reading?
Understanding the PHQ-9 Scoring System
The PHQ-9 was developed by Drs. Robert L. Spitzer, Janet B.W. Williams, and Kurt Kroenke as a module of the larger Patient Health Questionnaire. Its primary strength lies in its architecture: the nine items directly mirror the nine diagnostic criteria for major depressive disorder as outlined in the DSM-IV and DSM-5.
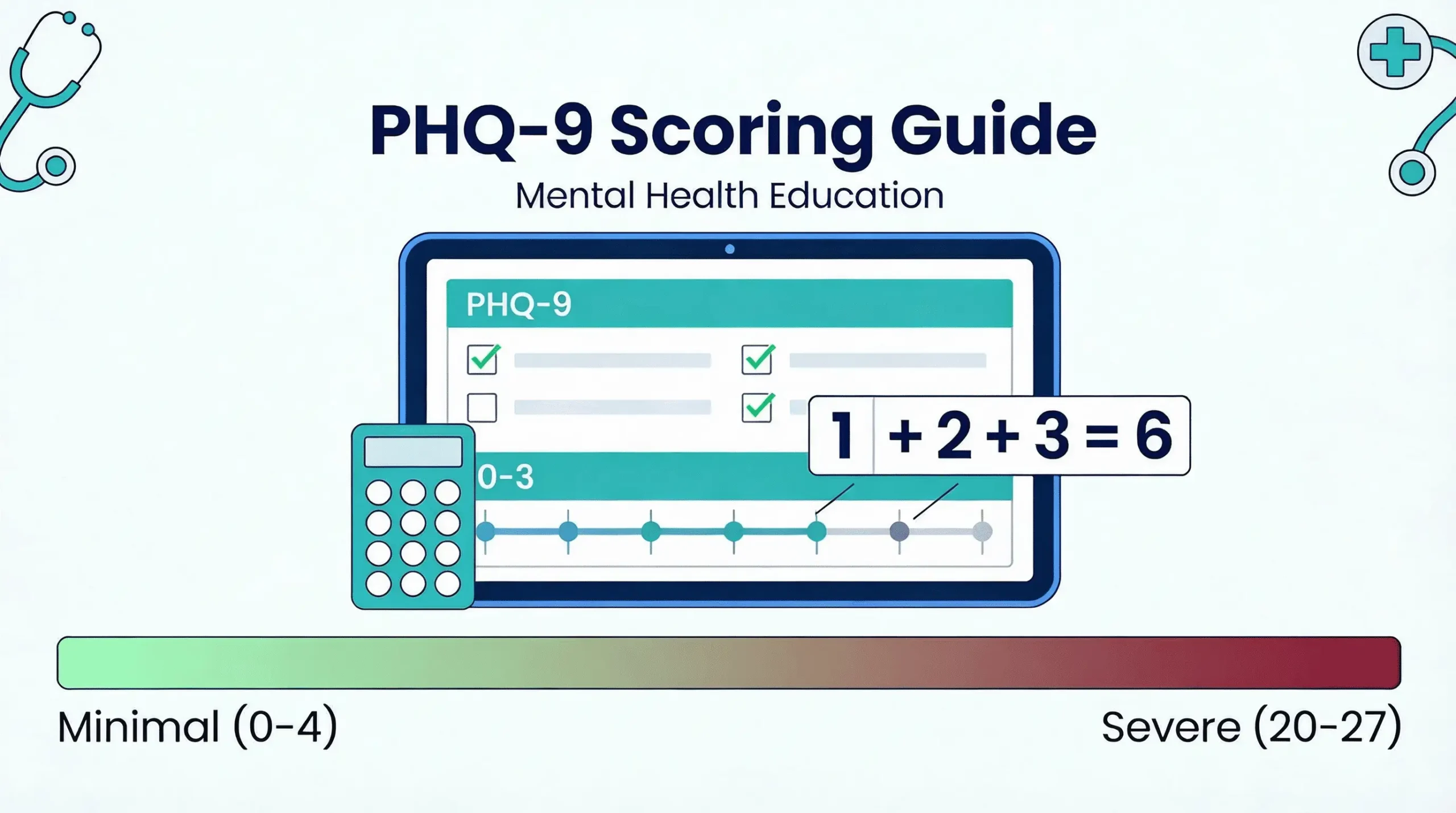
The 0–3 Likert Scale
The tool uses a simple numerical system to quantify the frequency of symptoms over a two-week “look-back” period. This specific timeframe is critical because it aligns with the temporal criteria required for diagnosing a major depressive episode. Patients rate each item using the following 4-point Likert scale:
- 0 Points: Not at all
- 1 Point: Several days
- 2 Points: More than half the days
- 3 Points: Nearly every day
The Functional Cluster of Symptoms
The nine items assess a patient’s experience across affective, cognitive, and somatic (physical) domains. These are categorized into functional clusters:
- Core Affective Symptoms: Anhedonia (item 1) and depressed mood (item 2).
- Somatic/Neurovegetative Symptoms: Sleep disturbance (item 3), fatigue (item 4), appetite changes (item 5), and psychomotor changes (item 8).
- Cognitive/Internal Symptoms: Negative self-concept (item 6), cognitive dysfunction or trouble concentrating (item 7), and thoughts of self-harm (item 9).
Step-by-Step Guide to Calculating the Total PHQ-9 Score
Calculations for the PHQ-9 are designed to be completed rapidly. In fact, many digital platforms like phq9test.com automate this process to ensure accuracy and completion.
- Step 1: Assign Point Values : Review the patient’s responses for items 1 through 9. Each “check” or selection corresponds to the numerical value (0, 1, 2, or 3) listed at the top of the column. Ensure that you are only looking at the first nine questions for the primary severity score.
- Step 2: Sum the Total: Add the scores for all nine items together. The resulting “Total Score”, also known as the Severity Score, will range from 0 to 27. A higher score indicates a higher symptom burden and greater depression severity.
- Step 3: Handling Missing Data (The Prorating Protocol): One of the most common hurdles for beginners is encountering a questionnaire where a patient has skipped an item. According to the American Psychiatric Association (APA) guidelines, you can still calculate a valid score if only one or two items are missing.
The Prorating Formula: For instance, if a patient answers eight items with a total sum of 12 points but leaves one blank, you multiply 12 by 9 (108) and divide by 8, resulting in a prorated total of 13.5 (rounded to 14).
Critical Limit: If three or more items are left blank, the score is considered invalid. The patient should be encouraged to complete the missing sections to ensure the data is clinically useful.
Interpreting the Severity: What the Numbers Mean
Once you have reached a total score, you must place it into a severity category. These categories help clinicians decide on the appropriate “Treatment Action Logic”.
PHQ-9 Severity Ranges and Clinical Actions
- 0–4: Minimal to None. At this level, treatment is generally not indicated. Clinical monitoring is usually sufficient unless symptoms persist.
- 5–9: Mild Depression. This range often warrants “watchful waiting.” Clinicians should provide education and self-care resources, then repeat the assessment in one month.
- 10–14: Moderate Depression. Often referred to as the “gray zone,” these patients may or may not meet the full criteria for a diagnosis. Clinicians should develop a treatment plan that may include counseling, psychotherapy, or pharmacotherapy (medication).
- 15–19: Moderately Severe Depression. Active treatment is typically initiated here, often utilizing a combination of psychotherapy and medication.
- 20–27: Severe Depression. This level requires the immediate initiation of pharmacotherapy. If the patient shows severe impairment, an expedited referral to a mental health specialist or psychiatrist is recommended.
Clinical “Red Flags” and Special Items
While the total score is helpful, beginners must learn to look at one item independently of the 0–27 sum which is item 9.
Item 9: The Suicide Risk Screen
Item 9 asks the patient about thoughts that they would be “better off dead” or of “hurting yourself in some way”. Because of the high clinical risk, any positive endorsement (a score of 1, 2, or 3) requires an immediate clinical response.
Research shows that patients who report these thoughts “nearly every day” (score 3) are 5 to 8 times more likely to attempt suicide within 30 days compared to those who report no such thoughts. If a patient scores above 0 on Item 9, staff should facilitate a “warm handoff” to a licensed professional for a full risk assessment, which includes evaluating the patient’s intent, plan, and access to means.
Scoring for Adolescents (PHQ-A)
While the standard PHQ-9 is validated for those 12 and older, a modified version called the PHQ-A is preferred for patients aged 11–17. The scoring mechanics (the 0–3 scale) remain identical, but the content is adjusted for developmental nuances.
Key Adolescent Adaptations
- Irritability: Items 1 and 2 are modified to include “feeling irritable,” as youth often express depression through irritability rather than sadness.
- School Context: Item 7 asks about trouble concentrating on “school work” rather than general reading.
- Dysthymia Screen: The PHQ-A often includes a specific question asking if the patient has felt sad or depressed for most days over the past year to screen for chronic depression (dysthymia).
The Diagnostic Algorithm: Syndrome vs. Severity
Beginners often confuse the Severity Score with a Diagnostic Algorithm.
- Severity Score (0–27): This is a continuous scale measuring the “burden” of symptoms. A cut-off of 10 or higher is used to “flag” patients who need further evaluation.
- Diagnostic Algorithm: To suggest a formal diagnosis of Major Depressive Disorder (MDD), a patient must endorse a specific pattern:
- At least one of the first two items must be a 2 or 3.
- A total of five or more of the nine items must be a 2 or 3 (except Item 9, which counts if it is a 1, 2, or 3).
Clinical studies show that the simple cut-off score of 10 is actually more sensitive than the complex algorithm for identifying cases in primary care. Therefore, most clinics use the score of 10 to trigger an interview and then apply the algorithm to confirm the diagnosis.
Tracking Progress with Measurement-Based Care
The ultimate value of the PHQ-9 is realized when it is used longitudinally. By re-administering the tool every 2 to 4 weeks (or 4 to 6 weeks depending on the setting), clinicians can objectively track if a patient is responding to treatment.
Defining Response and Remission
| Change in PHQ-9 Score | Clinical Interpretation | Recommended Action |
| Drop of points | Adequate Response | Maintain current treatment; follow up in 4 weeks. |
| Drop of 2–4 points | Inadequate Response | Consider increasing dose or psychotherapy intensity. |
| Drop of 0–1 point | No Response | Increase dose, switch meds, or add psychotherapy. |
The goal of acute treatment is remission, defined as a PHQ-9 score of less than 5. If a patient fails to achieve a 50% reduction in their score after two adequate treatment trials, a formal psychiatric consultation is recommended.
Mastering the Mechanics
Scoring the PHQ-9 is more than just summing nine numbers; it is about understanding the clinical logic that underpins each symptom. By using the total score to grade severity and closely monitoring high-risk responses on Item 9, you can provide a standardized, objective, and responsive level of care.
Always remember that while the PHQ-9 is a powerful screening tool with high diagnostic accuracy, it is not a replacement for a clinician’s evaluative role. Factors like bereavement, medical mimics (like thyroid issues), and bipolar disorder can influence scores and must be ruled out during a professional clinical interview.
Frequently Asked Questions
What is the PHQ-9 scoring range?
The PHQ-9 scoring range is 0-27. Each of the 9 questions is scored from 0 (not at all) to 3 (nearly every day), and all scores are added together to get the total.
How do you calculate the PHQ-9 score?
Add up the scores from all 9 questions. Each question is rated 0-3 based on how often symptoms occurred over the past two weeks. The sum of all responses gives you the total PHQ-9 score.
What is a normal PHQ-9 score?
A score of 0-4 is considered minimal or no depression and falls within the normal range. Scores of 5 or higher indicate some level of depressive symptoms requiring attention.
What does a PHQ-9 score of 10 mean?
A score of 10 indicates moderate depression (10-14 range). This suggests clinically significant symptoms that may require treatment such as counseling, follow-up monitoring, or antidepressant medication.
How is PHQ-9 Item 9 scored differently?
Item 9 (thoughts of self-harm) is scored the same way (0-3) but requires special attention. Any score above 0 on Item 9 indicates suicide risk and requires immediate safety assessment and intervention.
What is PHQ-9 prorating and when is it used?
Can the PHQ-9 diagnose depression?
No, the PHQ-9 is a screening tool, not a diagnostic instrument. A score of 10 or higher suggests probable depression and indicates the need for a full clinical evaluation by a healthcare professional.
What PHQ-9 score indicates severe depression?
A score of 20-27 indicates severe depression. This level typically requires immediate treatment intervention, including medication, intensive therapy, or possible hospitalization.