The PHQ-9 demonstrates 88% sensitivity and 88% specificity at a cut-off score of 10 when validated against structured psychiatric interviews, making it one of the most accurate depression screening tools in clinical practice. The Patient Health Questionnaire-9 (PHQ-9) has become a global benchmark for identifying and grading the severity of major depressive disorder (MDD) in diverse healthcare settings. As both a diagnostic aid and psychometric monitoring tool, understanding PHQ-9 accuracy is essential for healthcare providers making high-stakes clinical decisions regarding pharmacotherapy and psychotherapy referrals. This comprehensive guide explores the psychometric foundations, population-specific variations, and clinical challenges associated with the PHQ-9’s diagnostic performance.
Prefer listening over reading?
What Makes PHQ-9 Accurate? Core Performance Metrics
Sensitivity and Specificity at Standard Cut-Offs
Research involving over 6,000 patients across primary care and obstetrics-gynecology settings established that a PHQ-9 cut-off score of 10 provides an optimal balance between detecting true cases and avoiding false positives. At this threshold, the tool demonstrates:
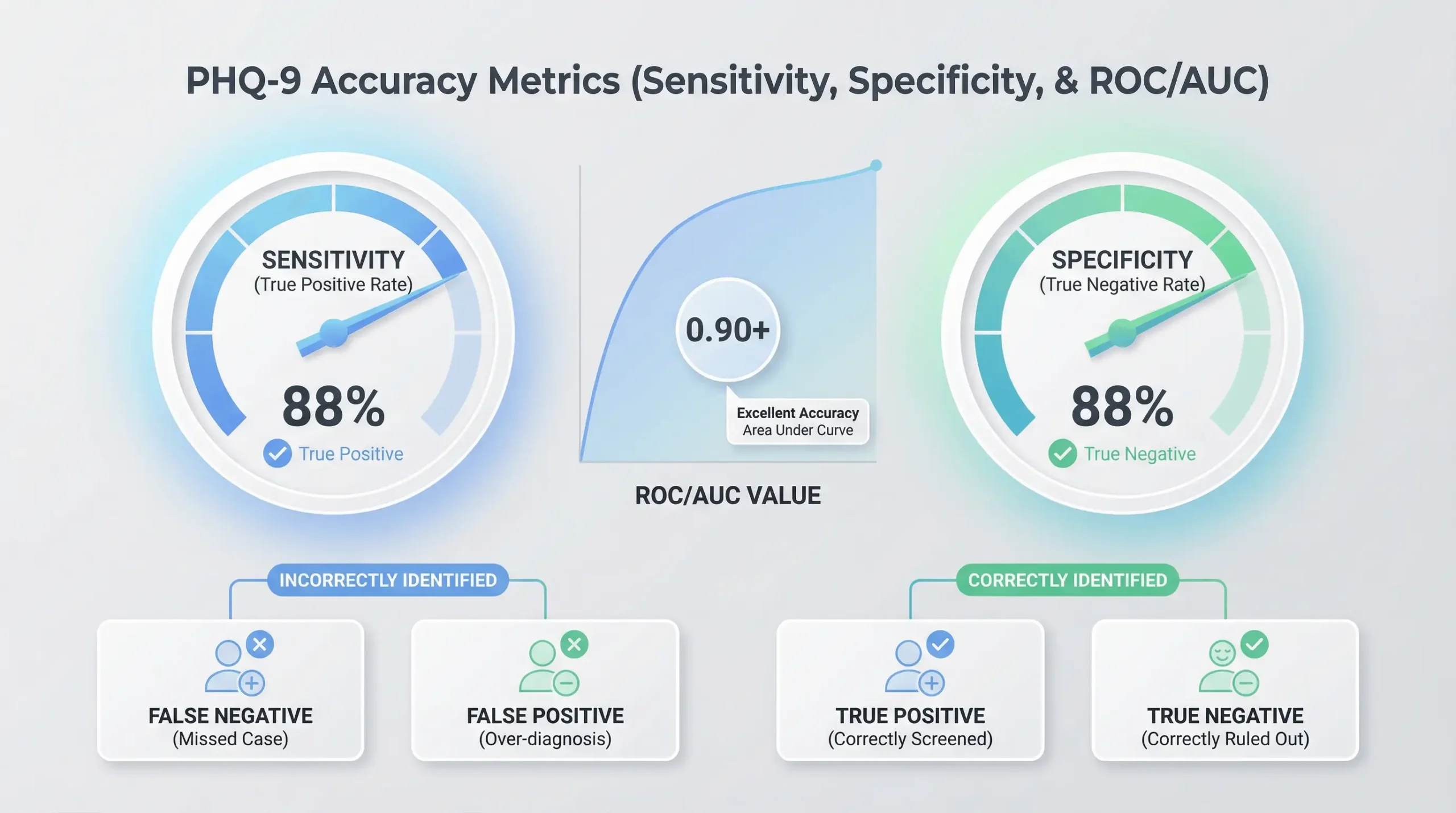
- Sensitivity: 88% – correctly identifies 88 out of 100 individuals with major depression
- Specificity: 88% – accurately excludes 88 out of 100 individuals without the disorder
These performance metrics were established through comparison with “gold standard” structured psychiatric interviews, including the Structured Clinical Interview for DSM (SCID) and the Mini International Neuropsychiatric Interview (MINI). The balanced accuracy at the cut-off of 10 makes the PHQ-9 particularly valuable for primary care settings where both over-diagnosis and missed cases carry significant clinical consequences.
Area Under the Curve (AUC) and ROC Analysis
The PHQ-9’s discriminatory power is further validated through Receiver Operating Characteristic (ROC) analysis, which measures the tool’s ability to distinguish between patients with and without depression across all possible cut-off scores. The Area Under the Curve (AUC) typically ranges from 0.88 to 0.95, indicating excellent diagnostic accuracy. An AUC of 0.88 means the PHQ-9 has an 88% probability of correctly ranking a randomly selected depressed patient as having a higher score than a randomly selected non-depressed patient. Values above 0.80 are considered excellent for screening instruments, and the PHQ-9 consistently exceeds this benchmark across diverse populations and clinical settings.
Cut-Off Trade-Offs: Balancing False Positives and Negatives
Clinicians should understand the inherent trade-off when adjusting cut-off scores to match their clinical priorities:
- Lower cut-off (8-9): Maximizes sensitivity to approximately 95%, ensuring very few depressed patients are missed, but increases false positives requiring follow-up assessment
- Standard cut-off (10): Provides balanced 88% sensitivity and specificity for general screening
- Higher cut-off (15): Ensures specificity of 95%, minimizing false positives but potentially missing patients with moderate depression who still require treatment
The optimal threshold depends on the clinical context—emergency departments may prioritize sensitivity to avoid missing high-risk patients, while specialty mental health clinics may prefer higher specificity to reduce unnecessary referrals.
Reliability Measures: Internal Consistency and Stability
Cronbach’s Alpha Across Clinical Settings
The PHQ-9 exhibits high internal consistency, meaning its nine items reliably measure a single underlying construct of depression severity. Seminal validation studies reported:
- Cronbach’s alpha (α) of 0.89 in primary care settings
- Cronbach’s alpha (α) of 0.86 in specialty medical clinics
- McDonald’s omega (ω) of 0.87 in Peruvian hospital samples
Global validation studies have corroborated these results across diverse populations, with Lithuanian university students showing α of 0.86 and similar coefficients reported across Asian, European, and Latin American samples. Alpha values between 0.80 and 0.90 are considered optimal for clinical instruments, high enough to ensure reliability but not so high as to suggest redundancy among items. These consistent coefficients indicate that the nine items are highly interrelated and effectively capture the multifaceted nature of depressive symptoms.
Test-Retest Reliability Over Time
Stability is a hallmark of PHQ-9 accuracy, ensuring that score changes reflect genuine clinical improvement or deterioration rather than measurement error. Test-retest reliability has been measured at 0.84 when patients complete the questionnaire at their initial clinic visit and again within 48 hours under similar conditions. This high degree of temporal stability means:
- Scores remain consistent when a patient’s clinical state is unchanged
- A reduction of 5 points or more represents a clinically meaningful response to treatment
- The tool can be used confidently for longitudinal monitoring at every visit
Healthcare providers can trust that fluctuations in PHQ-9 scores over weeks or months genuinely reflect changes in depression severity, making it an invaluable tool for tracking treatment outcomes and adjusting therapeutic interventions.
Age-Specific Accuracy: Adjusting Cut-Offs by Population
PHQ-9 Performance in Adolescents (Ages 13-17)
While the PHQ-9 maintains high sensitivity in adolescent populations, the standard adult cut-off of 10 may lead to over-identification due to developmental factors and transient distress common in teenage years. Validation research provides age-specific recommendations:
- Optimal cut-off: 11 for general adolescent screening (sensitivity 89.5%, specificity 77.5%)
- Higher cut-off: 15-16 in acute psychiatric inpatient settings where symptom severity is elevated
- Item weighting: Cognitive symptoms like “feeling bad about yourself” show stronger diagnostic utility than somatic complaints in youth
A study of 442 adolescents found that the slightly elevated threshold of 11 maintains excellent sensitivity while reducing false positives associated with normative adolescent mood variability and stress reactions to academic or social pressures. Clinicians working with adolescents should be aware that transient developmental distress can mimic clinical depression, making the higher threshold more appropriate for this age group.
Geriatric Screening Considerations
In older adults, PHQ-9 accuracy is complicated by the “confounding” effect where physical symptoms of aging may overlap with somatic manifestations of depression. Validation in geriatric populations suggests nuanced cut-off strategies:
- Cut-off of 6: Highly sensitive (95%) for initial screening, minimizing missed cases
- Cut-off of 9: More effective for confirming depression and reducing false positives from medical comorbidities
- Specificity advantage: Meta-analyses show 5-12% higher specificity in geriatric cohorts compared to younger adults
Chilean primary care validation in adults aged 65-80 demonstrated that older patients who reach the threshold of 9 tend to present with clearer diagnostic signals, as age-related complaints like fatigue are less likely to be mistaken for depression when cognitive-emotional symptoms are also present. A two-stage approach—screening at 6, confirming at 9—may optimize detection while managing false positives in geriatric care.
Cross-Cultural Validation and Global Accuracy
The PHQ-9 has been translated into over 70 languages with remarkable cross-cultural stability. Scalar invariance testing confirms that the instrument generally measures the same depression construct across different cultural contexts, though important nuances exist:
- Measurement equivalence: Confirmed in China, India, Peru, and across European populations
- Item weight variations: Somatic expressions of distress (fatigue, sleep, appetite) are more prevalent in South Asian and some Hispanic cultures
- Cultural symptom presentation: Some cultures emphasize physical complaints over emotional distress, which can influence total scores
In rural Indian populations, researchers found that lower education levels and female gender were significantly associated with higher symptom severity, underscoring the need for culturally informed interpretation. Despite these variations, the PHQ-9’s core psychometric properties remain robust, and the standard cut-off of 10 performs well across most cultural groups when validated against structured interviews conducted in the local language.
Medical Comorbidities: When Physical Symptoms Inflate Scores
Diabetes and Cardiovascular Disease Patients
One of the greatest challenges for PHQ-9 accuracy is distinguishing genuine depression from physical symptoms caused by chronic medical conditions. Patients with Type 2 Diabetes (T2DM) or Coronary Heart Disease (CHD) frequently experience:
- Persistent fatigue and low energy (PHQ-9 Item 4)
- Sleep disturbances (PHQ-9 Item 3)
- Appetite changes (PHQ-9 Item 5)
- Concentration difficulties due to metabolic dysfunction (PHQ-9 Item 7)
These overlapping symptoms can artificially inflate PHQ-9 scores, leading to overestimation of depression prevalence. Research in specialized diabetes clinics recommends:
- Higher cut-off of 12 to maintain specificity of 80% in T2DM populations
- Lower cut-off of 5 for rapid primary care screening as a “first-step” to identify patients needing thorough clinical interview
- Emphasis on cognitive-affective items: “Feeling down, depressed, or hopeless” and “Little interest or pleasure” as more discriminating indicators
Clinicians should interpret elevated PHQ-9 scores in medically complex patients with caution, using the numerical result as a starting point for clinical conversation rather than a definitive diagnosis. A comprehensive assessment should include evaluation of disease control, medication side effects, and functional impairment beyond what the medical condition alone would explain.
Cancer Populations and Somatic vs. Cognitive Item
In oncology settings, the diagnostic weight of different PHQ-9 items varies significantly from general populations. A large study of 4,705 cancer patients identified distinct patterns:
- Highest diagnostic value: “Little interest or pleasure in doing things” (Item 1) and “Feeling down, depressed, or hopeless” (Item 2)
- Lower diagnostic value: Appetite changes, fatigue, and sleep disruption—which may result from chemotherapy, radiation, or disease progression
- Risk of underestimation: Removing somatic items entirely could miss patients with genuine depression whose cognitive-emotional symptoms are less pronounced
While somatic items are less discriminatory in cancer patients, they remain clinically relevant for identifying mild-to-moderate distress and should not be disregarded. The total PHQ-9 score still provides valuable information about overall symptom burden, but oncology care teams should prioritize clinical interviews for patients with elevated scores to distinguish depression from expectable cancer-related symptoms. Some researchers suggest using the PHQ-4 (items 1, 2, 15, and 19 from the full PHQ) as an alternative for cancer populations where somatic contamination is a major concern.
Scoring Methods Compared: Sum Score vs. Diagnostic Algorithm
Why Sum Scores Achieve Higher Sensitivity
The PHQ-9 was originally designed with a dual scoring system, but extensive research has demonstrated clear superiority of one method over the other:
Sum Score Method (0-27 points):
- Add all nine items (each rated 0-3)
- Use cut-off of ≥10 for major depression
- Sensitivity: 88%, Specificity: 88%
Diagnostic Algorithm Method (DSM-based):
- Requires 5+ symptoms at “more than half the days” or higher
- Must include Item 1 or Item 2 (core symptoms)
- Sensitivity: 57-61%, significantly lower than sum score
Individual participant data (IPD) meta-analyses involving tens of thousands of patients have conclusively shown that the algorithm approach misses nearly one-third of patients with confirmed major depressive disorder. The algorithm’s lower sensitivity stems from its categorical nature—patients with four severe symptoms plus moderate levels of others may have clear MDD but fail to meet the algorithmic threshold.
Clinical Workflow Implications
Based on this evidence, best practice recommendations include:
- Use sum scores for screening: Total the points and apply cut-off thresholds
- Reserve algorithms for research: When strict DSM criteria adherence is required for diagnostic homogeneity
- Interpret severity bands: Minimal (0-4), Mild (5-9), Moderate (10-14), Moderately Severe (15-19), Severe (20-27)
- Track numeric changes: A 5-point reduction indicates clinically meaningful treatment response
The sum score approach is faster, more sensitive, and provides continuous measurement of symptom severity that facilitates treatment monitoring. Clinicians should abandon the algorithm method for routine clinical practice in favor of the validated sum score thresholds.
PHQ-9 vs. Other Depression Screening Tools
Beck Depression Inventory-II (BDI-II) Comparison
The BDI-II is a 21-item self-report measure widely used in psychiatric research and specialty mental health settings. Both instruments demonstrate comparable psychometric properties:
Similarities:
- High internal consistency (α >0.85)
- Excellent test-retest reliability
- Similar responsiveness to clinical change over time
- Validated against structured diagnostic interviews
PHQ-9 Advantages:
- Brevity: 9 items vs. 21 items (2-3 minutes vs. 10 minutes administration time)
- DSM alignment: Items directly correspond to DSM-5 MDD criteria
- Public domain: Free to use without licensing fees
- Primary care optimization: Designed specifically for high-volume medical settings
BDI-II Advantages:
- Greater granularity for measuring subtle changes in specialized psychiatric treatment
- More comprehensive coverage of cognitive symptoms
- Longer research track record in clinical trials
For busy primary care workflows where time efficiency is critical, the PHQ-9’s brevity makes it more practical while maintaining equivalent diagnostic accuracy. The BDI-II remains valuable in specialty psychiatric settings where the additional items provide more detailed phenotyping of depressive symptoms.
Hospital Anxiety and Depression Scale (HADS-D) Comparison
The HADS was designed specifically to avoid confounding from somatic symptoms in medical populations by excluding items about fatigue, sleep, and appetite. Comparative studies reveal important differences:
Case Detection Rates:
- PHQ-9 typically identifies twice as many moderate-to-severe cases as HADS-D
- This reflects the PHQ-9’s inclusion of somatic items and generally lower cut-off threshold
Interpretations of Divergence:
- Higher sensitivity view: PHQ-9 captures depression that HADS misses by excluding somatic symptoms
- Over-detection view: PHQ-9 over-identifies depression in medically ill patients due to symptom overlap
Clinical Implications:
- In populations with minimal medical comorbidity (young adults, psychiatric outpatients), PHQ-9 and HADS show closer agreement
- In chronic illness populations, the choice depends on clinical priorities—cast a wide net (PHQ-9) or prioritize specificity (HADS-D)
- Some clinicians use both: HADS for initial screening, PHQ-9 for treatment monitoring
The evidence suggests the PHQ-9’s somatic items, while potentially problematic in some medical populations, provide valuable information about total depressive burden and should not be eliminated entirely. Adjusting cut-offs (as discussed earlier) is preferable to switching instruments.
Item 9 and Suicide Risk Screening
Sensitivity vs. Specificity for Suicidal Ideation
PHQ-9 Item 9—”Thoughts that you would be better off dead or of hurting yourself in some way”—serves a critical safety function distinct from depression severity assessment. Unlike other items, any positive endorsement (score of 1, 2, or 3) is clinically significant and requires immediate follow-up.
Performance Characteristics
- High sensitivity for identifying patients with suicide risk
- Lower specificity compared to specialized instruments like the Columbia-Suicide Severity Rating Scale (C-SSRS)
- Over-identification tendency: PHQ-9 casts a wider net, flagging patients who may have passive thoughts without active planning or intent
Research demonstrates that Item 9 functions as an excellent primary screen but must be followed by comprehensive safety assessment. A positive response indicates the need for:
- Consideration of immediate safety planning or higher level of care
- Detailed inquiry about frequency, intensity, and duration of thoughts
- Assessment of specific plans, means, and intent
- Evaluation of protective factors and access to lethal means
Clinical Protocol for Positive Item 9 Responses
Best practices for managing positive Item 9 endorsements include:
- Immediate assessment: Never defer suicide risk evaluation to a future visit
- Direct questioning: Use clear, specific language to assess suicide plans and intent
- Documentation: Record the complete safety assessment in clinical notes
- Collaborative safety planning: Develop written plan with patient including warning signs, coping strategies, crisis contacts, and means restriction
- Follow-up intensity: Schedule more frequent monitoring for patients with active suicidal ideation
Important distinction: A patient who scores 1 on Item 9 (“several days”) with passive death wishes requires different intervention than a patient scoring 3 (“nearly every day”) with active planning. The PHQ-9 identifies the need for assessment but does not replace comprehensive suicide risk evaluation by a qualified clinician.
Item 9 should never be the sole basis for determining suicide risk level, but any positive score must trigger a mandatory safety protocol regardless of the patient’s total PHQ-9 score.
Clinical Best Practices for Maximizing PHQ-9 Accuracy
The PHQ-9 is one of the most rigorously validated instruments in mental health assessment, but its effectiveness is maximized when clinicians integrate numerical scores with professional judgment and contextual awareness. Evidence-based recommendations include:
Population-Specific Cut-Offs
- Adolescents (13-17 years): Use cut-off of 11 to account for developmental mood variability
- Older adults (65+ years): Screen at 6, confirm at 9 to balance sensitivity and specificity
- Medical comorbidities: Consider cut-off of 12 in diabetes, heart disease, and chronic pain populations
- Oncology patients: Emphasize cognitive-affective items (1 and 2) over somatic symptoms
Scoring Method Selection
- Always use sum scores (0-27 range) rather than diagnostic algorithms for screening
- Rely on total point count to determine severity and need for treatment
- Track score changes longitudinally—a 5-point reduction indicates clinically meaningful response
- Interpret scores within severity bands: Mild (5-9), Moderate (10-14), Moderately Severe (15-19), Severe (20-27)
Item 9 Mandatory Protocols
- Conduct suicide risk assessment for any Item 9 endorsement, regardless of total score
- Do not rely on Item 9 alone—use specialized instruments for comprehensive evaluation
- Document safety planning and follow-up protocols in medical record
- A score of 0 on Item 9 does not definitively rule out suicide risk in high-risk populations
Longitudinal Monitoring Strategies
- Administer PHQ-9 at every visit during active treatment to track progress
- Use score trajectories to guide treatment intensification or de-escalation decisions
- Combine PHQ-9 data with functional assessment and patient-reported improvement
- Consider two-stage screening: PHQ-2 for initial detection, full PHQ-9 for positive screens
Cultural and Contextual Considerations
- Be aware that somatic symptom emphasis varies across cultural groups
- Consider using interpreter services for non-English speakers rather than relying solely on translations
- Recognize that stigma may lead to under-reporting in some populations
- Supplement screening with clinical interview to understand symptom meaning and impact
By integrating these evidence-based practices, healthcare providers can maximize the PHQ-9’s already impressive accuracy and bridge the gap between undetected depression and life-changing treatment. The tool’s strength lies not just in its psychometric properties but in its practical application within a comprehensive, patient-centered approach to mental health assessment and monitoring.
Frequently Asked Questions
How accurate is the PHQ-9 for diagnosing depression?
The PHQ-9 demonstrates 88% sensitivity and 88% specificity at a cut-off score of 10 when validated against structured psychiatric interviews. Its Area Under the Curve (AUC) ranges from 0.88 to 0.95, indicating excellent diagnostic accuracy for major depression screening.
What is the best cut-off score for the PHQ-9?
The optimal cut-off is 10 for general adults, but should be adjusted to 11 for adolescents, 6-9 for older adults, and 12 for patients with diabetes or heart disease to account for developmental factors and physical symptom overlap.
Should I use the PHQ-9 sum score or diagnostic algorithm?
Always use the sum score method (0-27 range). Research shows the sum score achieves 88% sensitivity compared to only 57-61% for the diagnostic algorithm method. Sum scores are more sensitive and better for clinical screening.
Is the PHQ-9 reliable over time?
Yes, the PHQ-9 has excellent test-retest reliability of 0.84 and high internal consistency (Cronbach’s alpha 0.86-0.89). This ensures that score changes reflect genuine clinical improvement rather than measurement error, making it ideal for tracking treatment progress.
How accurate is PHQ-9 Item 9 for suicide risk?
Item 9 is highly sensitive for identifying suicide risk but has lower specificity compared to specialized tools like the C-SSRS. Any positive endorsement (score 1-3) requires immediate follow-up with comprehensive suicide risk assessment—it’s an excellent screener but not a diagnostic tool.
Does the PHQ-9 work accurately across different cultures?
Yes, the PHQ-9 has been validated in over 70 languages with consistent psychometric properties. Scalar invariance testing confirms it measures the same depression construct across cultures, though somatic symptoms may be emphasized more in South Asian and some Hispanic populations.
Is the PHQ-9 accurate for patients with chronic medical conditions?
The PHQ-9 can overestimate depression in patients with diabetes, heart disease, or cancer due to overlapping physical symptoms like fatigue and sleep changes. Use higher cut-offs (12+) or emphasize cognitive-affective items (feeling down, loss of interest) for better accuracy.
How do I know if a patient’s PHQ-9 score has meaningfully improved?
A reduction of 5 points or more indicates clinically significant improvement in response to treatment. Administer the PHQ-9 at every visit during active treatment to track progress and guide clinical decision-making about medication or therapy adjustments.